Breast cancer continues to be the most often diagnosed malignancy among Indian women and a significant factor in cancer-related mortality. This study examines the reasons behind India's persistently elevated breast cancer mortality rates, despite increasing awareness and enhancements in healthcare infrastructure. Utilizing GLOBOCAN 2022 data, we examined age-stratified incidence and death trends and performed a Pareto analysis to determine the age groups that significantly impact the national illness burden. A comparative descriptive analysis of Mortality-to-Incidence Ratios (MIR) across India, North America, the United Kingdom, and South Korea was conducted to investigate global differences in cancer outcomes. The results show that women aged 35 to 79 make up the vast majority of breast cancer deaths in India. The MIR goes up continuously with age, which shows that there are long delays in finding the disease, unequal access to modern treatments, and ongoing problems with cancer registry reporting. The three high-income regions, on the other hand, had much lower MIR values. This shows how well systematic screening, early diagnosis, and integrated care pathways work, even though they are not yet fully in place in India. Pareto study showed that 85% of breast cancer diagnoses and deaths come from three main age categories: 35–49, 50–64, and 65–79. This shows which groups should be the focus of national screening and intervention programs. The paper also talks about the new possibilities of 3D bioprinting, which may make tumor models that are physiologically realistic, drug screening with high accuracy, and individualized solutions for reconstructive surgery after a mastectomy. Combining these biotechnological developments with public health policies could help India lower its breast cancer burden and make sure that everyone has better clinical results.
| Published in | Journal of Cancer Treatment and Research (Volume 13, Issue 4) |
| DOI | 10.11648/j.jctr.20251304.18 |
| Page(s) | 164-168 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Cancer, Breast Cancer, India, Mortality-to-Incidence Ratio (MIR), 3D Bioprinting
Age Group | Incidence | Mortality | ASR (Incidence) | ASR (Mortality) | MIR |
|---|---|---|---|---|---|
20-34 | 12087 | 3347 | 20.4 | 9.4 | 0.276 |
35-49 | 56219 | 20726 | 103.7 | 62.7 | 0.368 |
50-64 | 74752 | 38212 | 209.4 | 193.2 | 0.511 |
65-79 | 41102 | 28728 | 427.8 | 315.5 | 0.698 |
80+ | 16133 | 13944 | 869.8 | 383.8 | 0.864 |
Region | N | Mean (M) | SD | SE |
|---|---|---|---|---|
India | 5 | 0.544 | 0.239 | 0.107 |
North America | 5 | 0.152 | 0.103 | 0.046 |
UK | 5 | 0.192 | 0.138 | 0.062 |
South Korea | 5 | 0.168 | 0.166 | 0.074 |
MIR | Mortality Index Ratio |
ASR | Age Standardized Rate |
| [1] | Mathur, P., Sathishkumar, K., Chaturvedi, M., Das, P., Sudarshan, K. L., Santhappan, S., Nallasamy, V., John, A., Narasimhan, S., & Roselind, F. S. (2020). Cancer Statistics, 2020: Report from National Cancer Registry Programme, India. JCO Global Oncology, 6, 1063–1075. |
| [2] | Malhotra, G. K., Zhao, X., Band, H., & Band, V. (2010). Histological, molecular and functional subtypes of breast cancers. Cancer Biology & Therapy, 10(10), 955–960. |
| [3] | Pramesh, C. S., Badwe, R. A., Borthakur, B. B., Chandra, M., Raj, E. H., Kannan, T., Kalwar, A., Kapoor, S., Malhotra, H., Nayak, S., Rath, G. K., Sagar, T. G., Sebastian, P., Sarin, R., Shanta, V., Sharma, S. C., Shukla, S., Vijayakumar, M., Vijaykumar, D. K.,... Sullivan, R. (2014). Delivery of affordable and equitable cancer care in India. The Lancet Oncology, 15(6), e223–e233. |
| [4] | Rijal, G., & Li, W. (2018). Native-mimicking in vitro microenvironment: an elusive and seductive future for tumor modeling and tissue engineering. Journal of Biological Engineering, 12(1). |
| [5] | Kulothungan, V., Ramamoorthy, T., Sathishkumar, K., Mohan, R., Tomy, N., Miller, G. J., & Mathur, P. (2024). Burden of female breast cancer in India: estimates of YLDs, YLLs, and DALYs at national and subnational levels based on the national cancer registry programme. Breast Cancer Research and Treatment, 205(2), 323–332. |
| [6] | Porter, P. (2008). “Westernizing” women’s risks? Breast cancer in Lower-Income countries. New England Journal of Medicine, 358(3), 213–216. |
| [7] | Sankaranarayanan, R. (2014). Screening for cancer in Low- and Middle-Income countries. Annals of Global Health, 80(5), 412. |
| [8] | Huang T, Jia CP, Jun Y, Sun WJ, Wang W. 3D bioprinting of a multicellular model for recapitulating the tumor microenvironment of breast cancer. Mater Today Adv. 2021; 12: 100176. |
| [9] | Dai, X., Cheng, H., Bai, Z., & Li, J. (2017). Breast cancer cell line classification and its relevance with breast tumor subtyping. Journal of Cancer, 8(16), 3131. |
| [10] | Neufeld, L., Yeini, E., Pozzi, S., & Satchi-Fainaro, R. (2022). 3D bioprinted cancer models: from basic biology to drug development. Nature Reviews. Cancer, 22(12), 679–692. |
| [11] | Chaji, S., Al-Saleh, J., & Gomillion, C. T. (2020). Bioprinted three-dimensional cell-laden hydrogels to evaluate adipocyte-breast cancer cell interactions. Gels, 6(1), |
| [12] | Mu, X., Zhang, J., & Jiang, Y. (2021). 3D printing in breast reconstruction: from bench to bed. Frontiers in surgery, 8, 641370. |
| [13] | Mayer, H. F., Coloccini, A., & Viñas, J. F. (2024). Three-dimensional printing in breast reconstruction: current and promising applications. Journal of Clinical Medicine, 13(11), 3278. |
| [14] | Datta, P., Dey, M., Ataie, Z., Unutmaz, D., & Ozbolat, I. T. (2020). 3D bioprinting for reconstituting the cancer microenvironment. NPJ precision oncology, 4(1), 18. |
| [15] | González-Callejo, P., Vázquez-Aristizabal, P., García-Astrain, C., de Aberasturi, D. J., Henriksen-Lacey, M., Izeta, A., & Liz-Marzán, L. M. (2023). 3D bioprinted breast tumor-stroma models for pre-clinical drug testing. Materials Today Bio, 23, 100826. |
APA Style
Rajeev, M., Bachani, P. (2025). Examining India's Breast Cancer Mortality Incidence Disparities and 3D Bioprinting's Potential. Journal of Cancer Treatment and Research, 13(4), 164-168. https://doi.org/10.11648/j.jctr.20251304.18
ACS Style
Rajeev, M.; Bachani, P. Examining India's Breast Cancer Mortality Incidence Disparities and 3D Bioprinting's Potential. J. Cancer Treat. Res. 2025, 13(4), 164-168. doi: 10.11648/j.jctr.20251304.18
AMA Style
Rajeev M, Bachani P. Examining India's Breast Cancer Mortality Incidence Disparities and 3D Bioprinting's Potential. J Cancer Treat Res. 2025;13(4):164-168. doi: 10.11648/j.jctr.20251304.18
@article{10.11648/j.jctr.20251304.18,
author = {Meghala Rajeev and Pooja Bachani},
title = {Examining India's Breast Cancer Mortality Incidence Disparities and 3D Bioprinting's Potential},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {4},
pages = {164-168},
doi = {10.11648/j.jctr.20251304.18},
url = {https://doi.org/10.11648/j.jctr.20251304.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251304.18},
abstract = {Breast cancer continues to be the most often diagnosed malignancy among Indian women and a significant factor in cancer-related mortality. This study examines the reasons behind India's persistently elevated breast cancer mortality rates, despite increasing awareness and enhancements in healthcare infrastructure. Utilizing GLOBOCAN 2022 data, we examined age-stratified incidence and death trends and performed a Pareto analysis to determine the age groups that significantly impact the national illness burden. A comparative descriptive analysis of Mortality-to-Incidence Ratios (MIR) across India, North America, the United Kingdom, and South Korea was conducted to investigate global differences in cancer outcomes. The results show that women aged 35 to 79 make up the vast majority of breast cancer deaths in India. The MIR goes up continuously with age, which shows that there are long delays in finding the disease, unequal access to modern treatments, and ongoing problems with cancer registry reporting. The three high-income regions, on the other hand, had much lower MIR values. This shows how well systematic screening, early diagnosis, and integrated care pathways work, even though they are not yet fully in place in India. Pareto study showed that 85% of breast cancer diagnoses and deaths come from three main age categories: 35–49, 50–64, and 65–79. This shows which groups should be the focus of national screening and intervention programs. The paper also talks about the new possibilities of 3D bioprinting, which may make tumor models that are physiologically realistic, drug screening with high accuracy, and individualized solutions for reconstructive surgery after a mastectomy. Combining these biotechnological developments with public health policies could help India lower its breast cancer burden and make sure that everyone has better clinical results.},
year = {2025}
}
TY - JOUR T1 - Examining India's Breast Cancer Mortality Incidence Disparities and 3D Bioprinting's Potential AU - Meghala Rajeev AU - Pooja Bachani Y1 - 2025/12/26 PY - 2025 N1 - https://doi.org/10.11648/j.jctr.20251304.18 DO - 10.11648/j.jctr.20251304.18 T2 - Journal of Cancer Treatment and Research JF - Journal of Cancer Treatment and Research JO - Journal of Cancer Treatment and Research SP - 164 EP - 168 PB - Science Publishing Group SN - 2376-7790 UR - https://doi.org/10.11648/j.jctr.20251304.18 AB - Breast cancer continues to be the most often diagnosed malignancy among Indian women and a significant factor in cancer-related mortality. This study examines the reasons behind India's persistently elevated breast cancer mortality rates, despite increasing awareness and enhancements in healthcare infrastructure. Utilizing GLOBOCAN 2022 data, we examined age-stratified incidence and death trends and performed a Pareto analysis to determine the age groups that significantly impact the national illness burden. A comparative descriptive analysis of Mortality-to-Incidence Ratios (MIR) across India, North America, the United Kingdom, and South Korea was conducted to investigate global differences in cancer outcomes. The results show that women aged 35 to 79 make up the vast majority of breast cancer deaths in India. The MIR goes up continuously with age, which shows that there are long delays in finding the disease, unequal access to modern treatments, and ongoing problems with cancer registry reporting. The three high-income regions, on the other hand, had much lower MIR values. This shows how well systematic screening, early diagnosis, and integrated care pathways work, even though they are not yet fully in place in India. Pareto study showed that 85% of breast cancer diagnoses and deaths come from three main age categories: 35–49, 50–64, and 65–79. This shows which groups should be the focus of national screening and intervention programs. The paper also talks about the new possibilities of 3D bioprinting, which may make tumor models that are physiologically realistic, drug screening with high accuracy, and individualized solutions for reconstructive surgery after a mastectomy. Combining these biotechnological developments with public health policies could help India lower its breast cancer burden and make sure that everyone has better clinical results. VL - 13 IS - 4 ER -
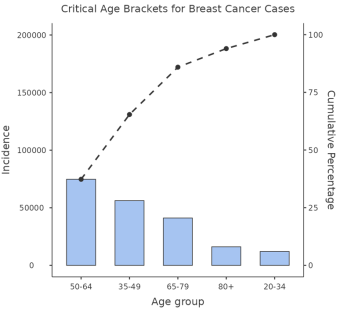
Figure 1. Pareto study of breast cancer rates in India by age group. The bar chart on the left displays the total number of new cases by age group, from highest to lowest. The line on the right shows the cumulative proportion, which reveals that three age groups (50-64, 35-49, and 65-79) make up 85.9% of all breast cancer cases.
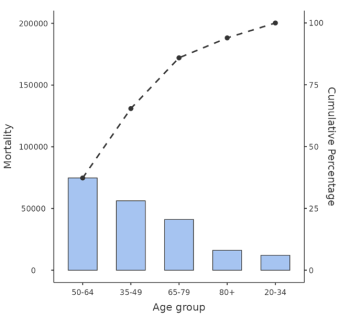
Figure 2. A Pareto study of breast cancer deaths in India by age group. The left y-axis shows the total number of deaths for each age group in order from highest to lowest. The right y-axis shows the cumulative percentage line, which shows that three age groups (50-64, 65-79, and 35-49) account for 83.5% of all breast cancer deaths. GLOBOCAN 2022 is the source of the data.

